



The Heart of the Matter: Myocarditis and COVID-19 Vaccines
A Parent's Guide to Understanding the Real Risks and Benefits of COVID-19 Vaccination (Particularly for Male Teens)
As parents, we're always looking out for our children's health and safety (thanks, Captain Obvious!). If you have a teenage son, you've likely seen alarming headlines about myocarditis - inflammation of the heart muscle - occurring after COVID-19 vaccination. These reports are understandably concerning and you might have some questions– so, we’re here to help.
Myocarditis sounds scary, and any risk to our children's hearts is something we take seriously. However, it's crucial to understand the full picture. While it's true that there is a small increased risk of myocarditis following mRNA COVID-19 vaccination, particularly in young males, the reality is far less alarming than some headlines might suggest. Most cases are mild and resolve quickly. More importantly, the risk of myocarditis - and other serious complications - is actually much higher if your child contracts COVID-19. Let's discuss.
What Is Myocarditis? Myocarditis refers to the inflammation of the heart muscle (myocardium). It can occur due to a viral infection, autoimmune response, or other causes—including, in rare cases, vaccination. Symptoms range from mild chest pain and fatigue to more severe outcomes like heart failure in extreme cases. In the context of COVID-19, both the virus and the vaccines designed to combat it have been associated with myocarditis. However, understanding the relative risk is crucial.
Recent large-scale studies, including nationwide and global population research, have provided crucial insights into the risk of myocarditis following COVID-19 vaccination. The highest risk group has been identified as males aged 12-30 years, with the risk peaking 1-14 days after the second dose of an mRNA vaccine.
Two major European studies quantified this risk, estimating excess myocarditis cases in young vaccinees (under 30) compared to unvaccinated individuals. For Comirnaty (Pfizer-BioNTech), estimates ranged from 0.26 to 0.57 per 10,000 vaccinations. For Spikevax (Moderna), the risk was higher, ranging from 1.3 to 1.9 per 10,000.
Importantly, the risk varies significantly across age groups. In children aged 5-11, myocarditis after vaccination is much rarer, with rates only slightly above background levels. No cases have been reported in children under 5 years old. For adults over 30 and the elderly, the risk remains only slightly elevated compared to baseline.
Follow-up studies by the CDC on affected individuals aged 12-29 have been encouraging. Most patients reported a return to pre-pandemic quality of life within 90 days, with 77-94% showing a return to normal biomarkers and imaging findings.
It's worth noting that myocarditis risk patterns in COVID-19 vaccination mirror those seen in viral infections. Males are more susceptible from childhood through young adulthood, while females face increased risk primarily post-menopause. This suggests that age and sex-related factors play a role in myocarditis susceptibility, both for infections and vaccinations.
Overview of mRNA Vaccines and Myocarditis Messenger RNA (mRNA) vaccines, like Pfizer and Moderna, use a small piece of genetic code to instruct cells to produce a protein that triggers an immune response.
P.S. Although COVID-19 vaccines were the first widespread use of mRNA technology, the science behind them has been in development for decades. Researchers began exploring mRNA-based therapies in the early 1990s, but it wasn't until the 2000s that breakthroughs in stabilizing mRNA and using lipid nanoparticles made the technology viable. Prior to the pandemic, mRNA vaccines were already being tested for diseases like rabies and influenza, allowing for their rapid adaptation to COVID-19.

This innovation has been key in controlling the spread of COVID-19. But as these vaccines rolled out globally, cases of myocarditis—primarily in younger males—began to emerge in public health surveillance databases.
The CDC and other health agencies have closely monitored this issue. Studies have shown that myocarditis occurs more frequently in males aged 16–30 years, particularly after the second dose of mRNA vaccines. Despite these reports, most cases have been mild and resolved quickly with minimal medical intervention.
Evidence of Myocarditis Following mRNA Vaccination
Here's a brief overview of the key findings from CDC data and related studies:
Myocarditis cases are more frequently reported in males, particularly those aged 16–30, after receiving the second dose of an mRNA vaccine.
Symptoms typically appear within a few days after vaccination, with chest pain, fatigue, and shortness of breath being the most common signs.
Most myocarditis cases post-vaccination have been mild and resolved with standard treatment, such as anti-inflammatory drugs.
While the risk of myocarditis after vaccination is real, it remains significantly lower compared to the risk posed by COVID-19 itself.

A Comparison Between Infection and Vaccination
Special thanks to our data visualization guru, Vrnda Aiyaswamy, for generating the following graphs to illustrate the risks of myocarditis following mRNA vaccination and SARS-CoV-2 infection. These graphs span data from January 2021 to January 2022, using sources from the CDC, PCORnet, and peer-reviewed studies.
Comparison of Incidents and Risk Ratio: Infection vs. Vaccination
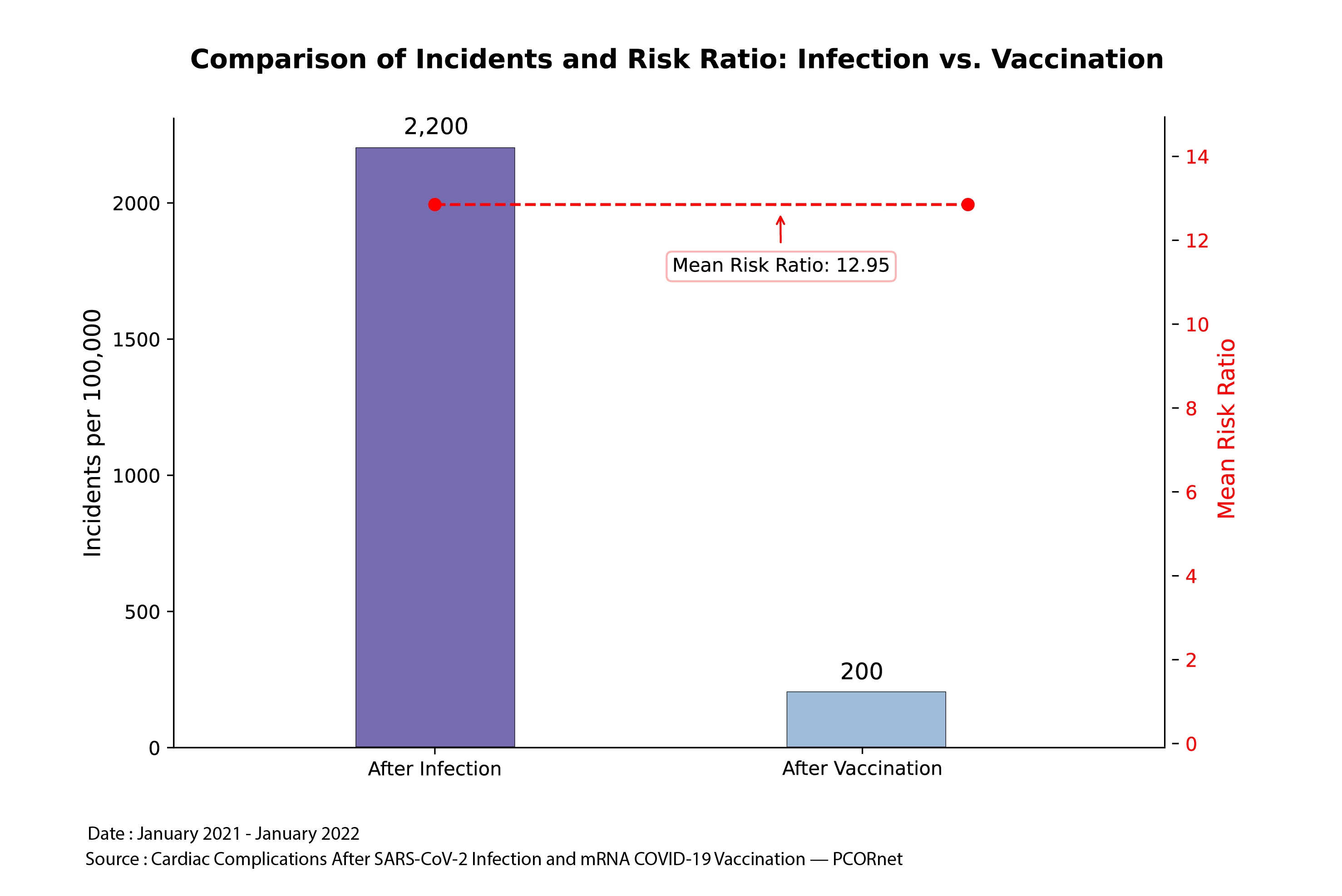
This graph offers a broad overview, demonstrating that the overall incidence of myocarditis after SARS-CoV-2 infection is dramatically higher than after vaccination.
The data reveals that the incidence rate of myocarditis following infection is 2,200 per 100,000, compared to just 200 per 100,000 after vaccination.
The mean risk ratio (12.95) shows that myocarditis is nearly 13 times more likely after infection than after vaccination.
Incidence of Myocarditis: SARS-CoV-2 Infection vs. mRNA COVID-19 Vaccination Among Males
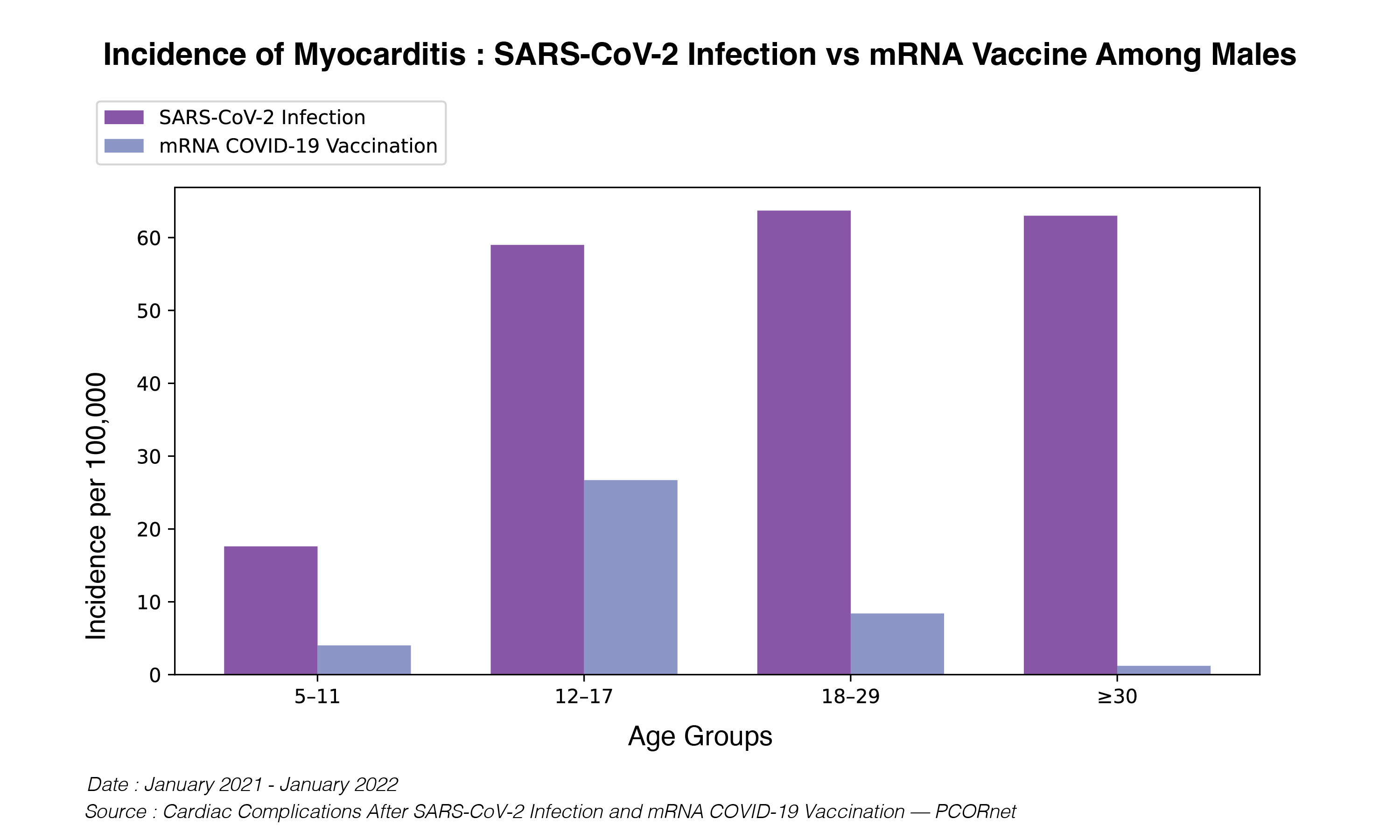
This graph focuses on males, the population most affected by post-vaccine myocarditis.
For males aged 12–17, the incidence rate of myocarditis following infection is about 55 per 100,000, while after vaccination, the rate is closer to 15 per 100,000.
In older age groups (18–29 and 30+), the trend remains similar, with infection posing a significantly higher risk of myocarditis than vaccination.
Myocarditis Risk Ratio by Age Group Among Males

See that red line labeled, “equal risk”? That represents the null hypothesis. At that value, the risk of myocarditis after vaccination is equal to the risk after infection. Anything above 1 reflects a HIGHER risk of myocarditis after infection compared to vaccination. As the number gets higher (and further away from the null value of 1) it reflects a higher magnitude of relative risk of myocarditis after infection compared to vaccination.
The risk ratio for myocarditis after infection is 8.4 times higher in males aged 18–29 compared to vaccination.
For those aged 30 and above, the ratio jumps to an astonishing 28.3 times higher.
Incidence of Myocarditis: SARS-CoV-2 Infection vs. mRNA COVID-19 Vaccination Among Females
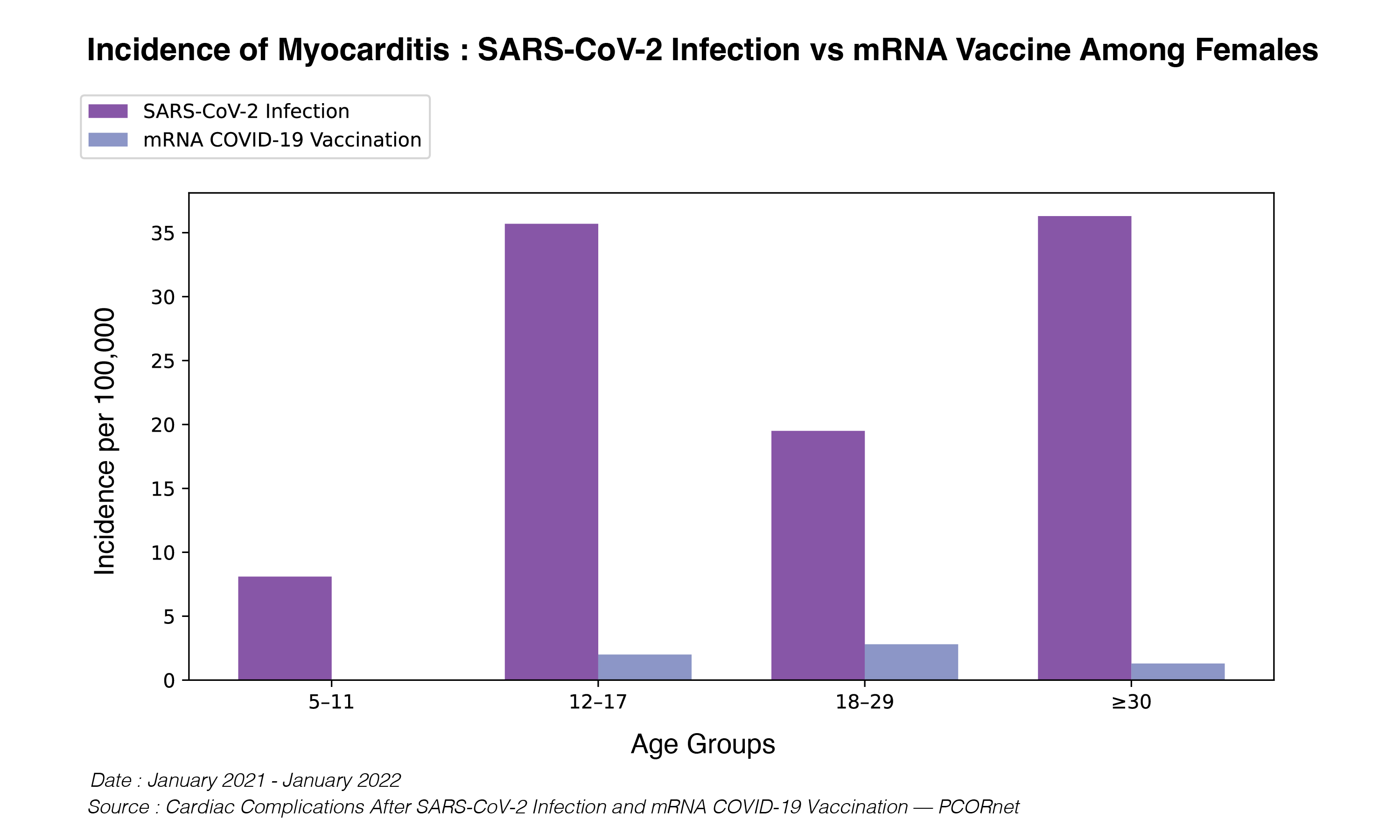
Although myocarditis primarily affects males, it can also occur in females.
Across all age groups, the incidence of myocarditis after infection is significantly higher than after vaccination.
For example, females aged 12–17 have an incidence rate of about 35 per 100,000 after infection, compared to fewer than 5 per 100,000 following vaccination.
Mechanism of Myocarditis
Although the precise mechanism behind vaccine-induced myocarditis isn't fully understood, researchers hypothesize that an immune response triggered by mRNA vaccines may lead to inflammation in susceptible individuals. One theory involves ACE2 receptors, present in heart cells and involved in SARS-CoV-2 viral entry, potentially becoming unintended targets during immune responses, leading to inflammation. Additionally, a recent article in Nature explores the role of transient immune dysregulation, including the activation of T-cells, macrophages, and pathways involving pro-inflammatory cytokines like IL-1 and IL-6, contributing to myocarditis risk.
Pfizer vs. Moderna: Is There a Difference? Emerging evidence indicates that the risk of myocarditis may be slightly higher after receiving Moderna's vaccine compared to Pfizer, especially in younger males. This distinction is worth noting but doesn't alter the overall conclusion that vaccination remains safer than infection. For example, one study found that the risk of myocarditis was higher following Moderna's second dose. However, even then, the overall risk remains low in comparison to the risk after contracting COVID-19.
What about Novavax?
For those concerned about mRNA vaccines, Novavax's protein-based vaccine, Nuvaxovid, offers an alternative. While it generally has milder side effects than mRNA vaccines, making it appealing for some individuals, it's important to note that it doesn't necessarily reduce the risk of myocarditis. In fact, limited data suggest the incidence might be slightly higher with Novavax, though more research is needed. Novavax provides good protection against severe COVID-19, but it may not generate the same robust T-cell response as mRNA vaccines. Additionally, its technology is slower to adapt to new variants. While Novavax is a viable option, especially for those who experience stronger reactions to mRNA vaccines, current evidence doesn't indicate that it offers significant advantages in terms of myocarditis risk or overall protection compared to mRNA vaccines. As with all COVID-19 vaccines, the risk of myocarditis following vaccination remains lower than the risk after COVID-19 infection itself.

(Ed Nirenberg of Deplatform Disease recently did a fantastic breakdown of Novavax. Highly recommend.)
Takeaways
As parents, it's natural to feel anxious when we hear about potential risks to our children's health. The reports of myocarditis following COVID-19 vaccination, especially in young males, have understandably raised concerns. However, when we look at the full picture, the data clearly shows that the benefits of vaccination far outweigh the risks.
Yes, there is a small risk of myocarditis following vaccination, particularly for teenage boys. But it's important to remember that:
These cases are rare and typically mild, resolving quickly with minimal treatment.
The risk of myocarditis - and other serious complications - is significantly higher if your child contracts COVID-19.
Vaccination provides crucial protection against severe COVID-19, which can have long-lasting health impacts.
As parents, we're always balancing risks and benefits for our children. In this case, the science is clear: vaccination is the safer choice. It not only protects your child but also helps safeguard more vulnerable members of our community.
xoxo,
Jess