

Is COVID-19 vaccine hesitancy affecting sentiment around other vaccines?
Is COVID-19 vaccine hesitancy affecting sentiment around other vaccines?
Polarization threatens to impact uptake of other routine vaccinations.
8 minute read
We know too well how transmissible and deadly COVID-19 can be, from epidemiological studies and our own lived experience in the prolonged pandemic. Yet we’ve also been empowered by our many tools of risk mitigation to reduce disease transmission and prevent adverse outcomes, risk mitigation with a proven history. Two years and two months in, let’s pause to explore one question still plaguing us: Is COVID-19 vaccine hesitancy affecting sentiment around other vaccines?
The COVID-19 anti-vaccine rhetoric is not new - indeed, it is the same messaging applied to other diseases eliminated by vaccines like polio, measles, etc. The anti-vaccine arguments never change, they are just reused according to which vaccine they are opposing. Indeed, there was even opposition during smallpox vaccination campaigns in the late 1700s and early 1800s. However, social media, politicization, and the other circumstances during the pandemic have exacerbated things.
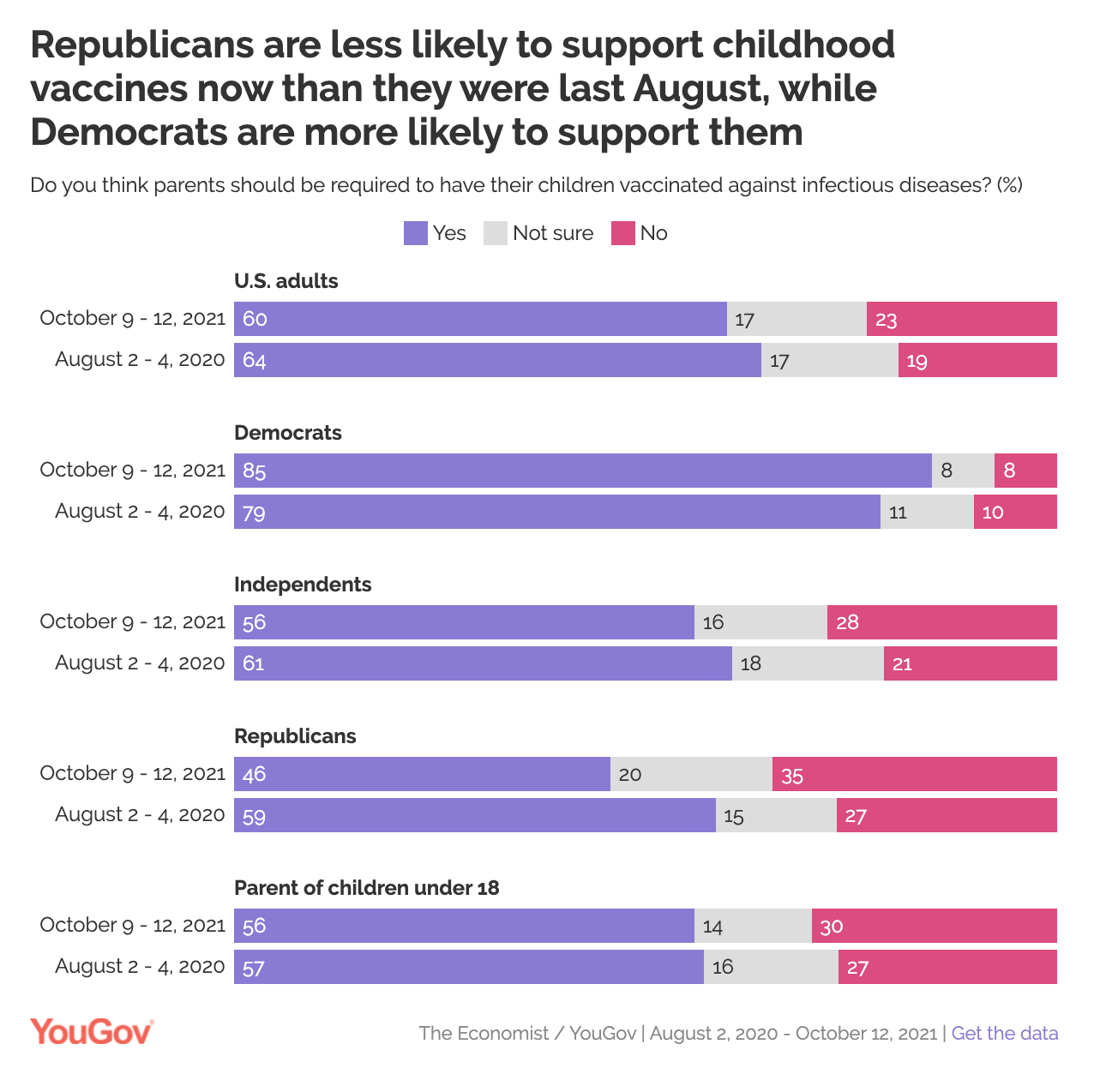
Remember: Mandated childhood vaccinations have been around in the U.S. since the 19th century. However, in the U.S., we now see a difference in vaccination sentiment that is divided along partisan lines. Yet the partisanship divide is pretty new. In the US, vaccination sentiment among Democrat and Republican affiliations has been trending in opposite directions starting in 2015. Republicans are expressing they’re less likely to support childhood vaccine requirements while Democrats are more likely to support childhood vaccines, according to pollsters.
In 2020, wild polio was declared eliminated in the African continent due to vaccination efforts. Just two years after vaccination campaigns and widespread vaccine uptake eliminated polio in Africa, a young girl was diagnosed with polio in the Malawi capital of Lilongwe. The diagnosis in January 2022 marked the first case of polio in Malawi in 30 years.
The reappearance of polio began just before the pandemic and likely worsened because health services were concentrated on pandemic related issues. However, pandemic-related vaccine hesitancy has also contributed to the decrease in vaccination following the reappearance of polio in Malawi. A polio vaccinator from the WHO found that around 50% of households in a village called Namazoma refused to get the vaccine with many parents worried it was a new oral COVID-19 vaccine.
After discussing the vaccine campaign with villagers, all households with family members home to meet with the vaccinators agreed to give the vaccine to their children
This demonstrates the far reaching effects of vaccine misinformation and how rumors surrounding the COVID-19 vaccine can negatively impact other public health issues
There is good news though: since the diagnosis of the young girl with polio in Malawi in January 2022, organizers have launched a mass vaccination campaign. Regional neighbors Zambia, Mozambique, Tanzania, and Zimbabwe have joined the effort.
Beyond outbreaks and anti-vaccine rhetoric, some unsettling policies around vaccination are emerging across the US. In July 2021, the Tennessee Department of Health announced it will halt all adolescent vaccine outreach for all diseases. In April 2020, Republicans in Colorado voted in opposition of any vaccination requirements. Indeed, there is legislation in many states across the country geared at eliminating long-standing public school vaccination requirements that have kept many deadly and debilitating illnesses under control for decades.
But the news isn’t all bad - although the number of vaccinations fell at the beginning of the pandemic due to suspended well-child visits and fears of being exposed at health facilities, parents' intentions to vaccinate their children against influenza increased 15.8% during the COVID-19 pandemic. However, the total number of vaccines administered decreased, influenced by factors like fear of being exposed to the virus at healthcare facilities and restrictions.
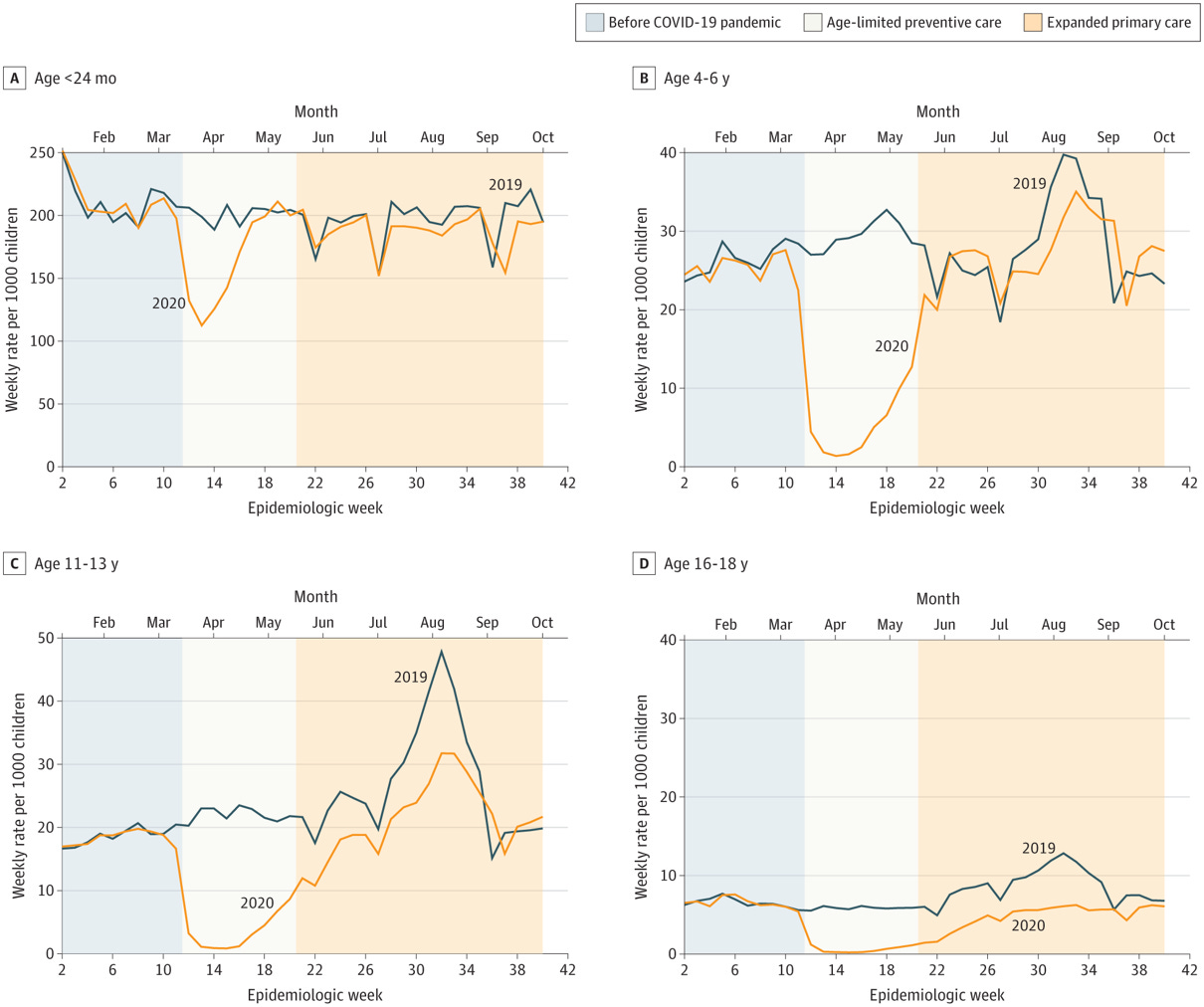
Vaccination trends in the US have changed over time. The general trend for the MMR vaccine experienced a steady rise since 1980; the combined MMR vaccine was licensed in 1971. However, a plateau occurred through late 1990s as a result of the damaging claims made by Andrew Wakefield regarding the false (and thoroughly debunked) link between MMR and autism. It was followed again by a steady rise again through 2019 (WHO), but a significant decrease in 2020 is noted in the JAMA article, which depict a clear gap in vaccination during COVID emergency in 2020:
It’s important to remember that decline in vaccination coverage can (and has) led to outbreaks of preventable diseases.
Let’s talk about measles, as an example:
Endemic measles was declared eliminated in the US in 2000 as a result of widespread vaccination campaigns and requirements for public schools. In December of 2015, there was an outbreak of measles at Disneyland when there were 45 cases in people who visited the park during the same period of time. The outbreak lasted 64 days total and there were 89 additional cases in California as the virus spread.
A study of 110 patients from California (identified by Feb 11, 2015), found 45% unvaccinated, 5% had 1 dose, 6% had 2 doses, 1% had 3 doses, 43% unknown/undocumented vaccine status. 28/37 unvaccinated patients (old enough to get the vaccine) refused due to personal beliefs.
In 18 studies referring to both outbreaks and annual summaries, there were 1416 cases of measles and 56.8% of which had not been vaccinated. This is particularly concerning due to the high level of transmissibility of the measles virus.
Remember: the R0 measures the number of people an infected person will infect and varies based on the disease. The R0 of measles can range from around 11-18, meaning one infected person can infect up to 18 other people. For context, the Delta variant of SARS-CoV-2 had an R0 of about 5. Because the R0 of measles is so high, vaccination rates need to reach around 95% of the population to have herd immunity. This also means the margin for error is low and seemingly small decreases in vaccination can have noticeable impacts.
Another study of measles outbreaks from Jan 1, 2000 (endemic measles eliminated) to November 30, 2015 found 56.8% of infected individuals were unvaccinated and 70.6% of unvaccinated individuals who were old enough to be vaccinated had non-medical exemptions. Following the outbreak, California changed its legislature and no longer allows vaccine exemptions on the basis of personal beliefs. Only health-related exemptions are now allowed (which are few and far between).
In 2018, a measles outbreak in New York mainly in Rockland County among Orthodox Jewish people was caused by an unvaccinated traveler with diagnosed measles from Israel where an outbreak was actively occurring with 3150 cases reported. There were 218 lab-confirmed cases and mainly affected children (median age 5 years). The coverage of measles vaccination among the schools in the outbreak area was 77%. The outbreak also spread to New Jersey with 33 cases. If even less people were vaccinated, this outbreak may have been less containable. This concern holds true now, as we have seen declines in MMR vaccination rates during the pandemic.
If we see increased vaccine hesitancy for routine vaccinations, it can get ugly for public health. People, including children, will die preventable deaths.
So what can we do to increase vaccine acceptance?
Community engagement, improved health and science education, and yes, governmental legislation can all impact this.
Educating people about vaccines’ effectiveness and the disease’s risk can increase vaccination uptake. Moreover, facilitating the vaccination process by minimizing barriers (better healthcare access and logistics) can help, too.
Studies on communication surrounding vaccines have found that that engaging in conversations about vaccination with hesitant parents led to higher rates of HPV vaccination in children.
Parents who were alerted that their child should receive the HPV vaccine were then shown a video to ease their concerns, a video to encourage them to get the vaccine, both videos, or neither video.
Survey results showed parents who only saw the “ease concern video” were more comfortable with their children getting the vaccine and parents who only saw the “encourage vaccination video” did not show less vaccine hesitancy.
The “ease concern video” addressed vaccine concerns whereas the “encourage vaccination video” was simply a strong recommendation from physicians to get the vaccine.
The study suggests that listening to and addressing people’s concerns is a more productive and effective way to reduce vaccine hesitancy compared to relying solely on recommendations and regulations. Note: we recently did a live Q&A with Immunize Virginia that sought to address many of these same concerns regarding the HPV vaccination.
Overall, we’re living in an era of increased hesitancy for routine vaccinations. It could be ugly - or get uglier - for public health. People, including children, will die preventable deaths. But as history has shown us too, it doesn’t have to be this way! Public agencies, health care providers, civil society, and even celebrities educating people about vaccines’ effectiveness and disease risk can inform and increase vaccination uptake. Our governments can help to minimize barriers such as providing better access to health care and improving infrastructure logistics. Some examples include increasing door-to-door vaccination, partnering with community organizations, and making vaccine counseling reimbursable for providers. These measures can positively affect vaccination uptake in our complicated context of vaccine hesitancy.
Collaborators and contributors:
Dr. Dharmi Desai, MD, MPH Student in Health Policy and Social Media Specialist, Yale School of Public Health
Kayla Steinberg, Digital and Social Media Strategist, Yale School of Public Health
Sam Hillier