

How does fetal development relate to pregnancy dating?
How does fetal development relate to pregnancy dating?
Embryological development and clinical timing of pregnancy differ.
A challenge surrounding scientific discussions of reproductive health is the fact that colloquialisms or ‘softened language’ are used. This leads to misunderstanding or misconceptions related to the physiological processes that occur.
As such, we thought it useful to provide a quick overview of embryology in the context of humans – using correct & scientific terminology. However, it’s also important to dissect the differences between embryological development and clinical dating of pregnancy.
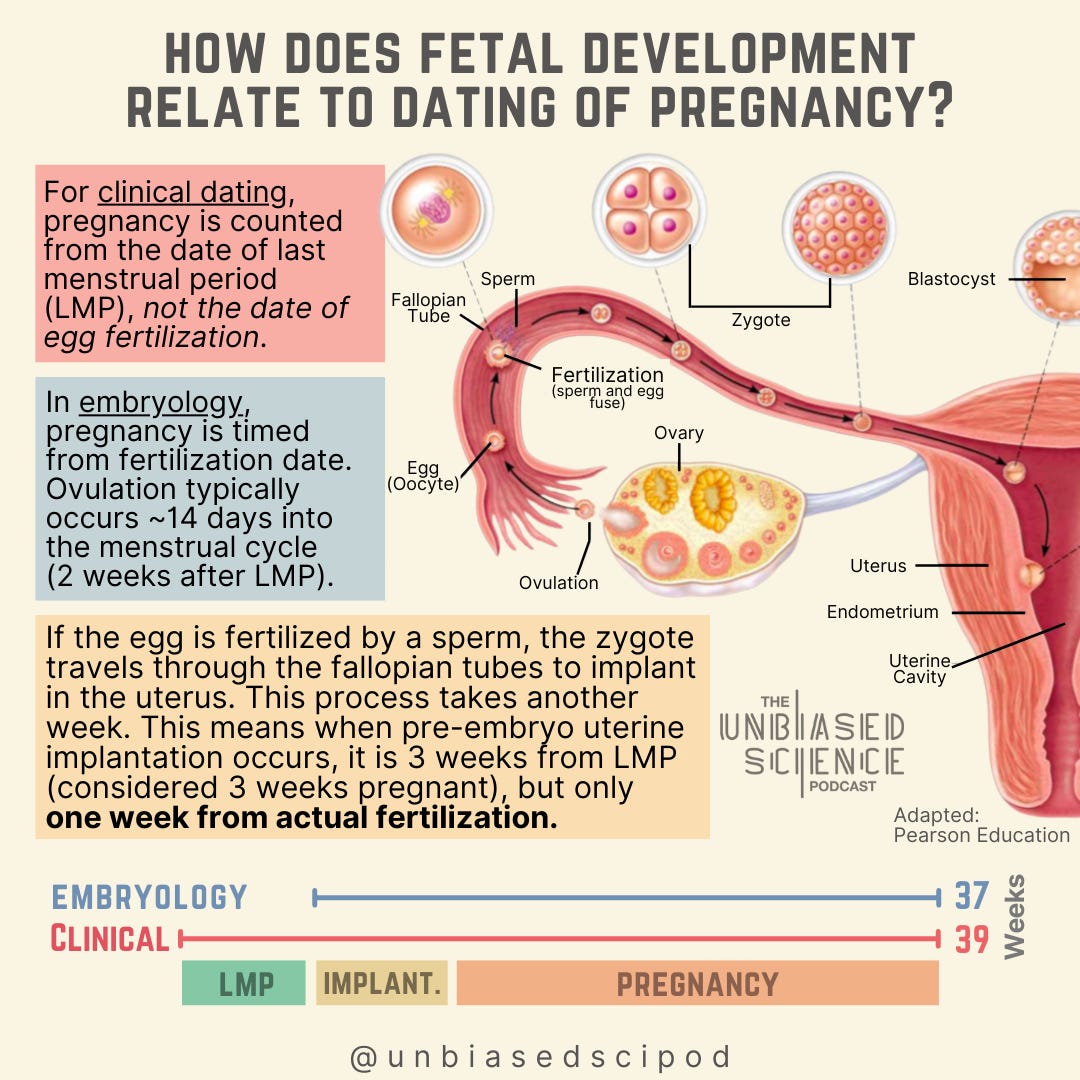
Clinical human gestation is ~39 weeks, divided into trimesters (3 month periods). However, embryological gestation is closer to 37 weeks. There is a 2 week difference between embryological determination of pregnancy and clinical determination of pregnancy. The reason for this? The menstrual cycle.
Clinical pregnancy is counted from the date of last menstrual period, not the date of fertilization, meaning there can be a substantial delay between fertilization and knowing about pregnancy.
This is because ovulation - or release of an egg from the ovary - occurs about 2 weeks into the menstrual cycle. In other words, ovulation occurs ~ 2 weeks after the last menstrual period (LMP).
Ovulation (release of an egg from an ovary) occurs ~2 weeks after the last menstrual period (LMP). From there, the egg enters the fallopian tube and, if fertilized by a sperm, becomes a zygote. After fertilization, rapid cell division occurs through cleavage forming a structure called a blastocyst. At this point the zygote is still traveling toward the uterus, which takes about a week.
Once the pre-embryo enters the uterus, it must successfully implant for pregnancy to progress. If implantation does not occur, or if the egg was never fertilized, the uterus will shed the lining and menstruation will occur.
This is the critical piece: fertilization occurs ~ 2 weeks after LMP.
From an embryological perspective, implantation into the uterus is 1 week after fertilization. From a clinical perspective, and how pregnancies are dated for medical purposes and for laws being passed banning abortion access, they are dated from LMP. That means when a pre-embryo is implanting into the uterus one week after fertilization, this would be considered 3 weeks pregnant for clinical (and legal) purposes.
This is done clinically because LMP is the most consistent method of dating a pregnancy, unless intrauterine insemination (IUI) or in vitro fertilization (IVF) is performed where fertilization date is known.
The first 2 weeks of pregnancy are the zygote period. A zygote is the cell produced by the union of an egg (ovum) and a sperm through fertilization. After fertilization, rapid cell division occurs during a process called cleavage, forming a structure called a blastocyst. This pre-embryo develops into the embryo. For clinical purposes, these 2 weeks would actually be considered weeks 3 and 4 of pregnancy. The first 2 weeks of clinical pregnancy would be the 2 weeks after the last menstrual period, where there is actually no pregnancy yet.
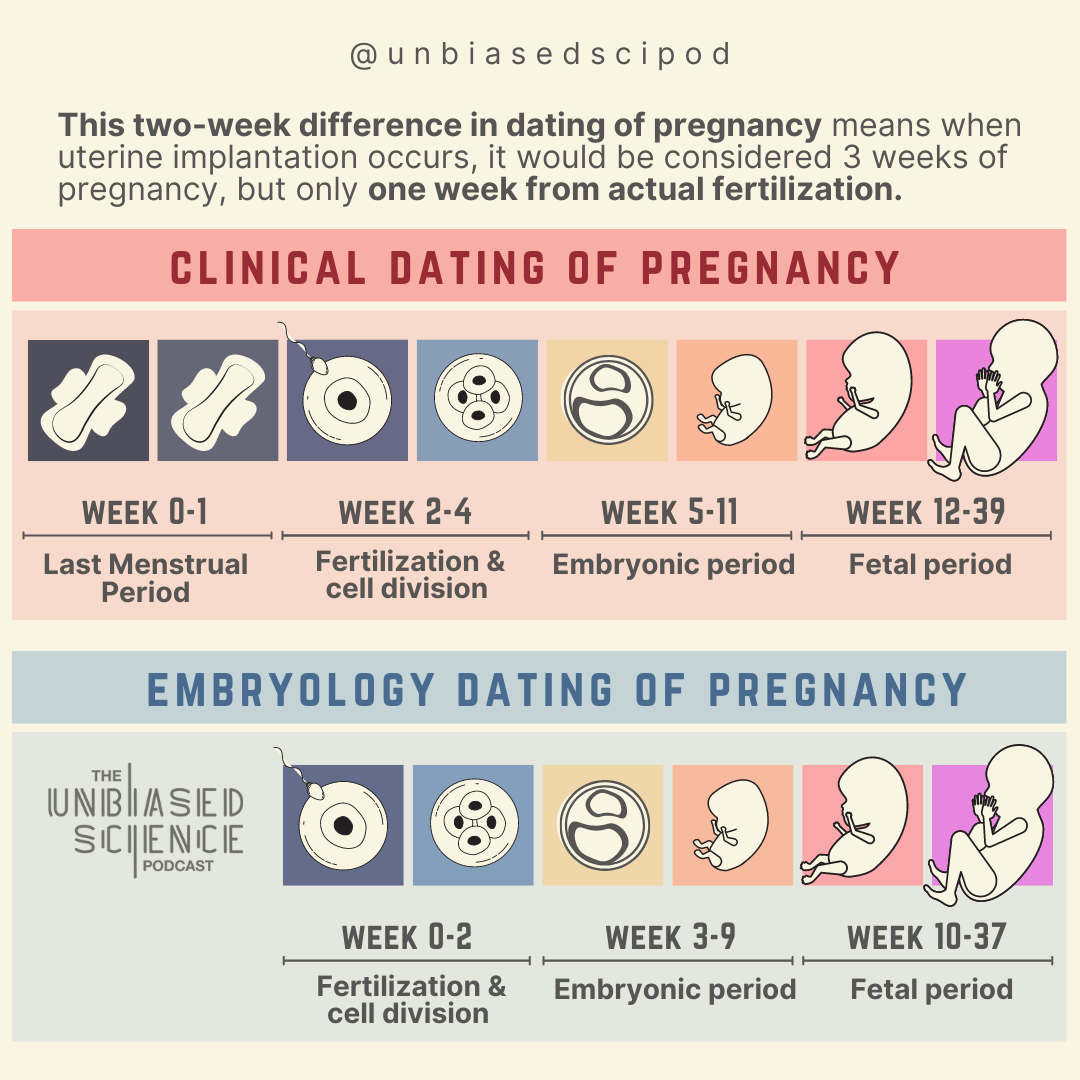
The embryonic stage is week 3 through week 9 (or clinically, weeks 5 through 11). This begins with a process called gastrulation, where the embryo divides, forms rudimentary tissue structures, and begins to differentiate into cell types that will form organ & anatomical systems.
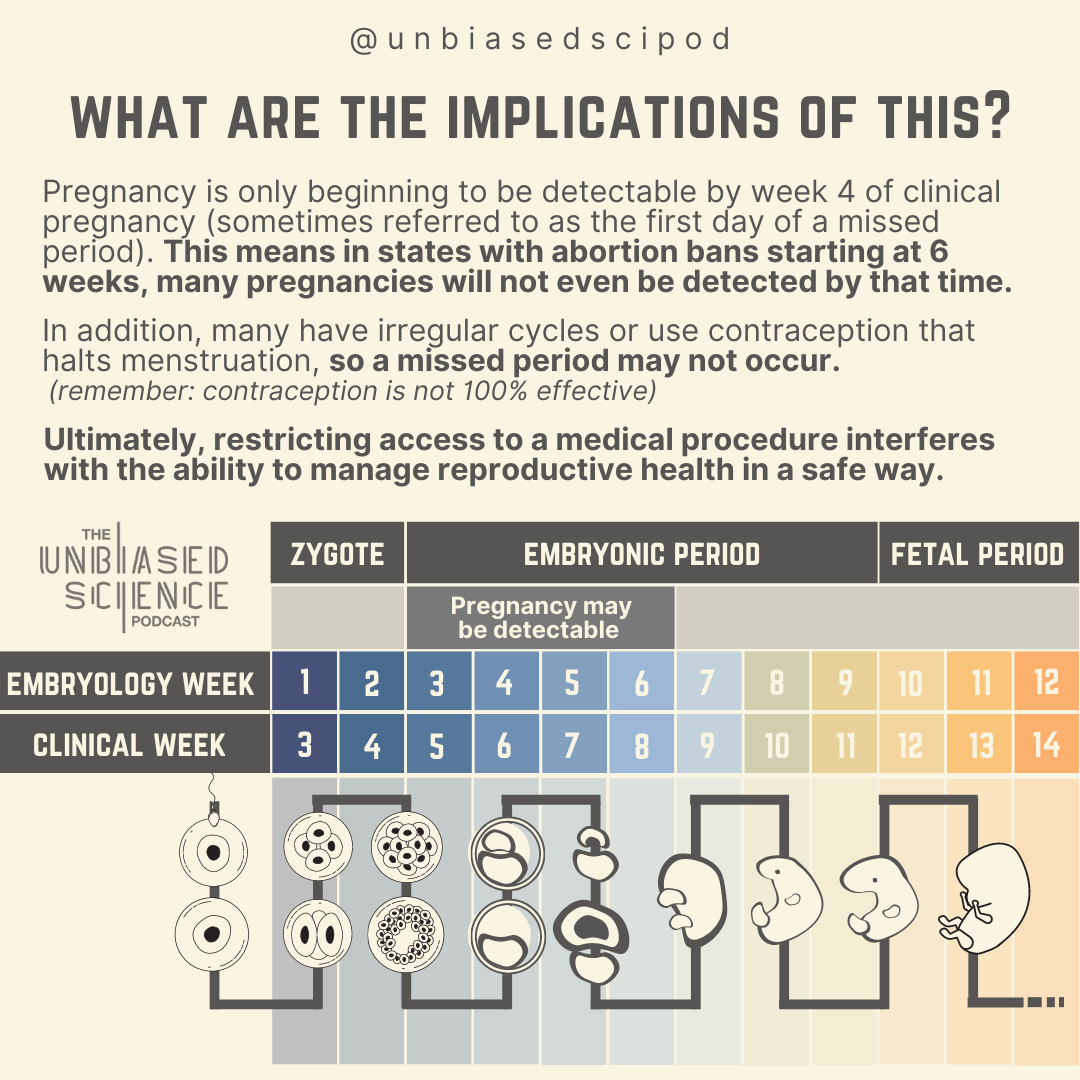
Depending on when during the menstrual cycle fertilization occurred, pregnancy *may* be detectable by week 2 (week 4 clinically), but most commonly by week 6. 33% of pregnancies are detected after week 6 (week 8 clinically).
Weeks 10 (week 12 clinically) through birth are the fetal period.
During this period, different tissue layers form functional structures. Electrical activity can be detected in cardiac cells that will eventually develop into the heart by week 20 of pregnancy. The brain continues to develop, which will ultimately control bodily functions. A fetus born from week 24 is considered viable, although very pre-term births require substantial medical intervention. During the third trimester, week 27 through birth, a fetus is considered viable, unless there are major developmental abnormalities.
Ultimately, ‘clinical pregnancy’ begins before an egg is even fertilized; accelerating the timeline by 2 weeks. As such, pregnancies are only starting to be detected by week 4 of clinical pregnancy (the first day of a missed period). In addition, many people do not have regular 28-day cycles, or are on contraception to prevent pregnancy that may halt menstruation (yes, you can still get pregnant on contraception, nothing is 100% effective).
As a result, laws restricting access to abortion after 6 weeks will have serious medical and public health implications for people trying to safely manage their reproductive healthcare.
Additional contributors