



An increase in cancer rates?
Possibly. But a recent study is being misused to spread undue fear.
Hundreds of messages have come pouring in about cancer and the things that might cause higher than typical cancer diagnosis trends. Recent headlines have again sparked concern that cancer rates are skyrocketing – particularly among younger adults (under the age of 50 years).
As a result, we are seeing an increase in claims both in traditional and social media outlets that certain factors (e.g., sugar, processed foods, pesticides, COVID-19 vaccines, etc) are CAUSING the increased rates of cancer. We want to explore this topic further and will focus on a 2023 study in particular that is often cited as the reason for concern.
What are the key elements of this study?
Study Focus:
Research Question: The study aims to analyze global trends in early-onset cancers (diagnosed between the ages of 14 to 49) from 1990 to 2019 - investigating incidence, deaths, risk factors, and the global burden of this disease.
Data Source: It uses the Global Burden of Disease (GBD) study. This massive research project collects and analyzes health data from around the world.
Key Findings:
Trend: Early-onset cancers (under the age of 50 years) are on the rise globally, especially since the mid-1990s.
Incidence of early-onset cancers is up 79.1% from 1990 to 2019
Deaths from early onset cancers are up 27.7% from 1990 to 2019
The study prediction models indicated that the age brackets between 40-44 and 45-49 will represent a significant proportion of the population affected by early-onset cancer morbidity and mortality in the next 10 years.
Cancer Types: The most significant increases were found in cancers of the breast, colon & rectum, esophagus, kidney, liver, gallbladder, pancreas, and stomach.
Breast, tracheal, bronchus, lung, stomach, and colorectal cancer have the highest mortality and disability-adjusted life years (DALY)
Nasal and prostate cancer have the fasted increasing trend
Liver cancer has had the sharpest decrease (Note: this could be due to hepatitis B vaccination mandates and the availability of effective treatments for hepatitis C)
One DALY represents the loss of the equivalent of one year of full health. DALYs for a disease or health condition are the sum of the years of life lost (YLLs) due to premature mortality and the years lived with a disability (YLDs) due to prevalent cases of the disease or health condition in a population.
Disparities:
The highest-burden regions and cancer types were high-middle and middle Socio-Demographic Index (SDI) regions.
SDI is the composite indicator of a location's socio-demographic developmental status strongly correlated with health outcomes. It is calculated by measuring:
Total Fertility Rate Under the Age of 25 (TFU25): This measures the average number of children a woman is expected to have before the age of 25.
Mean Education for Those Ages 15 and older (EDU15+): It reflects the educational attainment of the population aged 15 and above.
Lag Distributed Income (LDI) Per Capita: This considers the income distribution within the population.
Researchers use the SDI to understand how development status impacts health outcomes. It helps identify disparities and guide health interventions.
The SDI is calculated as the geometric mean of these three indices, resulting in a value between 0 and 1. Therefore, 0 corresponds to a theoretical minimum level of development relevant to health and an SDI of 1 represents a theoretical maximum level of development.
Risk Factors: The researchers linked early-onset cancer to several modifiable lifestyle factors and more:
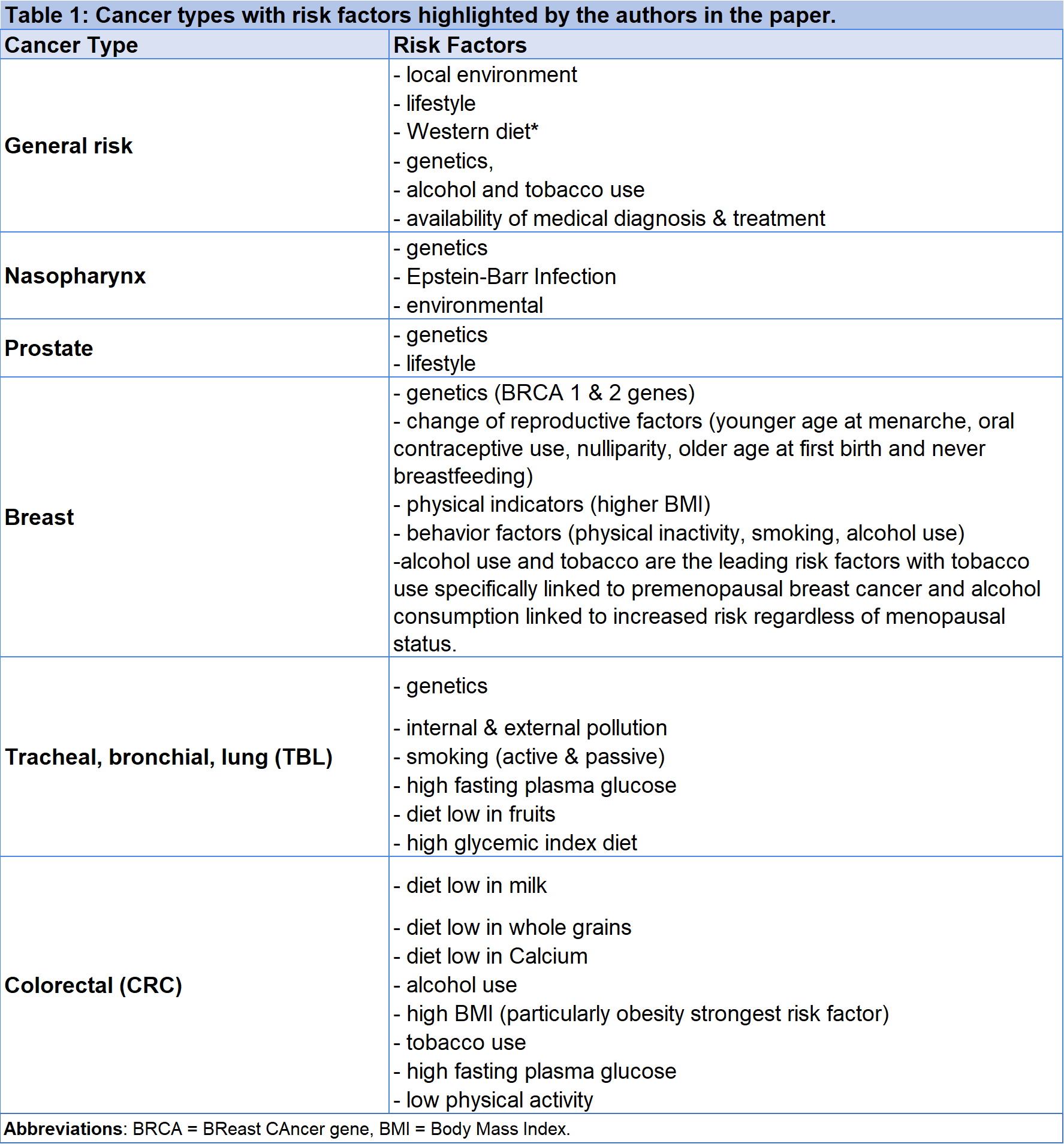
*Note: a major limitation of the study is that the data contained in many global cancer databases are insufficient to properly address the research question. The accuracy of GBD data is compromised by the quality of cancer registry data in different countries. Thus, the under-reporting and under-diagnosis in undeveloped countries may result in an underestimation of the incidences and deaths of early-onset cancer. While it is likely that a heavily obesogenic diet is a poor prognostic factor, the fact that Western countries are better at reporting in this database could skew this finding, it is important to view this finding with caution.
Modifiable risk factors seen consistently across cancer types:
Diet - “Western” diets, high glycemic index diets, diets high in red meat, high in sodium, and low in whole grains and fruits.**
Alcohol and Tobacco Use
Blood sugar dysregulation (e.g. diabetes, metabolic syndrome) and high fasting plasma glucose
Lack of physical activity
Obesity
Outdoor & indoor pollution
**Let’s discuss this particular finding regarding diet - Upon review, it is not clear how the authors calculated dietary risk in this specific paper. It doesn't appear to be referenced in their methods, but the supplemental data refers to this paper from 2020.
From this, it appears the GBD analyses of diet used a very different method of risk assessment for diet, calculating a "theoretical minimum risk exposure level (TMREL)" based on wider research (~44 systematic reviews). There may be a few issues with this:
First, the effect of the same dietary exposure is not homogenous across populations, unless for some well-established dietary risk factors (e.g., sodium).
This does appear to be evident in the main analysis of diet from the GBD, which showed regional variation in the % of DALYs attributable to diet.
As the present analysis is looking at temporal trends, we would want to be clear that this is truly reflected in the dietary data, i.e., that the correlations are with changes in diet over time.
Ultimately, most of the suggestions from the present study about diet are nothing new and have not raised anything controversial relative to the existing, wider literature.
Implications & Importance
Cancer isn't just a disease of older populations. We need to understand why young people are increasingly affected.
The strong link to lifestyle/modifiable factors means many of these cancers could be preventable and therefore puts focus on health promotion and early detection.
While the study suggests causes, we still need more in-depth studies on why early-onset cancer is rising and how best to address it.
This study is being taken out of context to spread panic and fear - here’s what you need to know:
Changing Screening Practices: Increased detection is due to better screening and could play a role in the rising incidence of some cancers, rather than an actual increase in the disease itself.
Data Quality: The GBD database relies on the quality of data provided by different countries. Underreporting or inaccurate diagnoses in some regions could skew the results.
Lack of Detail on Risk Factors: While the study links early-onset cancer to lifestyle factors, it often doesn't have granular data on individual patients. For example, it might broadly link to 'diet' but not know the specifics of each person's eating habits.
Observational Nature: This type of study identifies associations, not direct cause and effect. We cannot definitively say that specific lifestyle factors are directly causing this spike in cancer without more controlled studies.
Dr. David Robert Grimes, PhD Physics and Cancer Biology:
“The observational nature of this study is the biggest limitation, compounded by the quality of the data. There is no mechanistic model underpinning the findings, so there is no way to observe whether trends are just noise or means we need to conduct better quality studies to help solidify this understanding.”
Why does correlation versus causation matter?
Correlation does not equal causation. Just because two things seem linked (like processed food consumption and rising early-onset cancer rates) doesn't mean one directly causes the other. Here's why:
Confounding Factors: Other factors not considered in the study could be the true cause. For example, environmental pollution, genetics, etc.
Complexity of Disease: Cancer development is incredibly complex and likely involves multiple factors working together over time.
So what should I take away from this study?
This publication is in line with an even more recent study and interestingly both arrive at similar recommendations.
Key takeaways of that study:
The study found a 19.4% increase in cancers within 30-39 year olds since 2010.
Researchers looked at data from 17 National Cancer Institute Surveillance, Epidemiology, and End Results registries between January 1, 2010, and December 31, 2019, and found over 560,000 incidences of early-onset cancer.
Asian or Pacific Islander patients under 50 saw the biggest increases (32%) in cancer, while Hispanic patients had a 28% increase and Black patients had an almost 5% decline.
There was a 4.4% increase in early-onset cases among women, while men saw a 5% decline—researchers believe a spike in breast cancer may have caused the case to rise in women.
Breast cancer had the highest case rates while gastrointestinal cancers—including the appendix, colon, and bile duct—had the fastest-growing incidence rates, with a 15% increase in early-onset cases during this time.
Koh B, Tan DJH, Ng CH, et al. Patterns in Cancer Incidence Among People Younger Than 50 Years in the US, 2010 to 2019. JAMA Netw Open. 2023;6(8):e2328171. doi:10.1001/jamanetworkopen.2023.28171
A healthy lifestyle goes a long way in helping to reduce the incidence of early-onset cancers and is what we individually have control over.
Consume a more balanced and nutritious micronutrient diet
Eliminate tobacco use
Eliminate or at the least, reduce the intake of alcohol
Be more active as a sedentary lifestyle is harmful to many aspects of health
Manage and control blood sugar if you are pre-diabetic, diabetic, or have metabolic syndrome - work with your doctor, diabetic educator, or certified nutritionist
Tackle obesity and find healthy ways to lose weight - work with your doctor and certified nutritionists
Improve the quality and quantity of sleep
Avoid living in cities with high pollution rates
Reduce exposure to indoor pollution (e.g. asbestos, dust mites, chemicals, mildew, carbon monoxide, etc) by improving ventilation, using HEPA filters, reducing unnecessary chemicals in the house, and using indoor plants (they can help improve air quality naturally)
Preventive care is also important and our healthcare guidelines for early detection of cancer are constantly evolving with the science - always check with your doctor.
Diagnose and treat Helicobacter pylori infections if you have a history of stomach pain, reflux, and/or ulcers.
Discuss genetic testing with your doctor if you have a family history of certain cancers (e.g. breast cancer - BRCA 1 & 2)
Get your Hepatitis B vaccine to help prevent liver cancer and Human Papillomavirus (HPV) vaccines to help prevent cervical, vaginal, vulvar, throat, penile and anal cancers
Wear sunscreen and protect yourself from the sun - and get your skin & moles checked - especially if they change in any way
Discuss and get the recommended screenings appropriate for your age beginning around 40 years of age (see some recommendations below).
Screening recommendations for early detection of cancer (not exhaustive):
Prostate Specific Antigen (PSA) testing: While the CDC general guidelines recommend starting at age 50 for men at average risk of prostate cancer, PSA screening between the ages of 40 and 54 may be appropriate if:
Have at least one first-degree relative (such as a father or brother) who has had prostate cancer
Have at least two extended family members who have had prostate cancer
Are African American, an ethnicity that has a higher risk of developing more aggressive cancers
From 55 years onward, men benefit the most from PSA screening as it is when it is most likely to develop.
Breast cancer screening: The American Cancer Society (ACS) guidelines for women at average risk for breast cancer. For screening purposes, a woman is considered to be at average risk if she doesn’t have a personal history of breast cancer, a strong family history of breast cancer, or a genetic mutation known to increase the risk of breast cancer (such as in a BRCA gene), and has not had chest radiation therapy before the age of 30. (See below for guidelines for women at high risk.)
Women between 40 and 44 have the option to start screening with a mammogram every year.
Women 45 to 54 should get mammograms every year.
Women 55 and older can switch to a mammogram every other year, or they can choose to continue yearly mammograms. Screening should continue as long as a woman is in good health and is expected to live at least 10 more years.
All women should understand what to expect when getting a mammogram for breast cancer screening – what the test can and cannot do.
Clinical breast exams are not recommended for breast cancer screening among average-risk women at any age.
Women who are at high risk for breast cancer based on certain factors should get a breast MRI and a mammogram every year, typically starting at age 30.
Colorectal Cancer Screening:
The ACS recommends that people at average risk of colorectal cancer start regular screening at age 45.
Screening can be done either with a sensitive test that looks for signs of cancer in a person’s stool (a stool-based test), or with an exam that looks at the colon and rectum (a visual exam).
For screening, people are considered to be at average risk if they do not have:
A personal history of colorectal cancer or certain types of polyps
A family history of colorectal cancer
A personal history of inflammatory bowel disease (ulcerative colitis or Crohn’s disease)
A confirmed or suspected hereditary colorectal cancer syndrome, such as familial adenomatous polyposis (FAP) or Lynch syndrome (hereditary non-polyposis colon cancer or HNPCC)
A personal history of getting radiation to the abdomen (belly) or pelvic area to treat a prior cancer
People who are in good health and with a life expectancy of more than 10 years should continue regular colorectal cancer screening through the age of 75.
For people ages 76 through 85, the decision to be screened should be based on a person’s preferences, life expectancy, overall health, and prior screening history. People over 85 should no longer get colorectal cancer screening.
Cervical Cancer Screening:
The American College of Obstetrics and Gynecology (ACOG) Screening should begin at age 25 and end at age 65
The preferred screening method is an HPV test alone every 5 years.
Other acceptable screening methods are an HPV/Pap co-testing every 5 years or a Pap test alone every 3 years.
Screening is not recommended for those younger than 21 or older than 65 nor for those without a uterus and cervix (total hysterectomy) who had no history of high-grade cervical cancer lesions or cervical cancer.
This study adds to the growing awareness of early-onset cancer as a serious issue. It is a reminder to prioritize healthy choices (as detailed above) and to stay up-to-date on cancer screenings. However, we need more information to have a complete picture as there is considerable uncertainty over whether increases (and decreases) are real or artifacts of reporting bias, improved detection, and/or screening.
How do we know that the COVID-19 vaccines are not causing an increase in cancer diagnoses?

There is no evidence that COVID-19 vaccines are causing cancer at this time. This is a myth being perpetuated by a handful of people on social media who are well-known for providing misinformation about COVID-19 and vaccines. A recent multinational study of over 99 million patients in the Global Vaccine Data Network™ study aimed to evaluate the risk of adverse events of special interest (AESI) following COVID-19 vaccination from 10 sites across eight countries. They confirmed the pre-established safety signals for myocarditis, pericarditis, Guillain-Barre syndrome, and cerebral venous sinus thrombosis, but they have not noted findings specific to cancer thus far.
The American Cancer Society explains that the COVID-19 pandemic is expected to cause increased cancer mortality over the long term due to other more unfortunate reasons - delayed diagnoses, interruptions or alterations in potentially curative treatment, the possibility that some adults will abandon prior patterns of preventive care, and the expectation that millions of adults will remain unemployed and without health insurance.”
The good news is that significant efforts are being made across the world to monitor COVID-19 vaccines and their safety over time.
What’s the bottom line?
This study provides updated evidence that the incidence of early-onset cancers is increasing globally and is useful for prioritizing, funding, and conducting more robust clinical studies in this area.
It also highlights disparities that are worth exploring regarding the increase in early-onset cancer particularly for differing sociodemographic index regions, women, marginalized populations, and individuals less than 50 years of age. Further research is required to fully elucidate the reasons for these disparities.
This study also serves as a call to inform healthcare professionals about the increasing incidence of early-onset cancer, and investigations for future studies in cancer particularly in patients younger than 50 years.
For public health professionals and health care policymakers, this study serves as a call to action for further research into the various environmental and modifiable risk factors that may be associated with early onset cancers.
Most importantly, studies like this help us open a dialogue with patients about their risk of developing early onset cancer, understanding and tackling modifiable risk factors and encouraging them to utilize the healthcare tools we have available to reduce their risk and to detect cancers earlier.
Please be cautious not to misinterpret this and other studies to imply that certain things (e.g., pesticides, vaccines, etc.) are causing an increase in cancer diagnoses simply because of correlations between their use and cancer outcomes. When in doubt, harken back to this post which uses a bit of humor to illustrate this common logical fallacy.

Special thanks to Michelle Bridenbaker, Dr. David Robert Grimes, and Dr. Alan Flanigan for their contributions to this article.
Michelle Bridenbaker, RN, BSN, MS, MBA, is an accomplished and patient-focused senior leader with extensive experience transforming many aspects of medical/scientific affairs, health communication, and multichannel engagement across industry and healthcare. With a healthcare, toxicology, and communications background, Michelle has worked tirelessly to ensure patient safety and improved health outcomes and to empower and arm healthcare professionals with information that directly impacts patient care. In support of her passion for serving patients and healthcare professionals, she is active on scientific boards and volunteers as a consultant for various tech firms supporting healthcare, not-for-profit organizations, and in public health.
David Robert Grimes (PhD, CStat) is a scientist, broadcaster, and author of "The Irrational Ape - Why we fall for conspiracy theory, disinformation, and propaganda" (Simon & Schuster UK, US title: "Good Thinking - Why Flawed Logic Puts us all at Risk and How Critical Thinking Can Save the World - The Experiment publishing). He has a background in cancer science, mathematical modeling, and public understanding of science. He contributes to the Guardian, BBC, Scientific American, The Atlantic, and many other outlets, and is a CFI Fellow and Maddox prize winner. He is on Instagram at david_robert_grimes, Twitter (X) at @drg1985, and online at davidrobertgrimes.com
Alan Flanagan, Ph.D. The University of Surrey. IG: @thenutritionaladvocate
 | A guest post by
|